World Contraception Day 2022: Dr. Elsie Akwara and Dr. Venkatraman Chandra-Mouli report on the global situation of teenage pregnancies and childbearing
Looking back with satisfaction at the progress made in adolescent pregnancy and child bearing globally, and looking ahead at the enormous amount that yet needs to be done
By Dr. Elsie Akwara and and
Dr. Venkatraman Chandra-Mouli
Globally, the adolescent birth rate (ABR) has decreased from 64.5 births per 1000 women aged 15-19 years in 2000 to 42.5 births per 1000 women in 2021 (1 - UNDESA, 2021). However, rates of change have been uneven across regions, with the sharpest decline in South Asia (SA), and slower declines in the Latin American and Caribbean (LAC) and sub-Saharan African (SSA) regions. Although declines have occurred in all regions, SSA and LAC continue to have the highest rates globally at 101 and 53.2 births per 1000 women aged 15-19 years, respectively, in 2021 (1 - UNDESA, 2021).
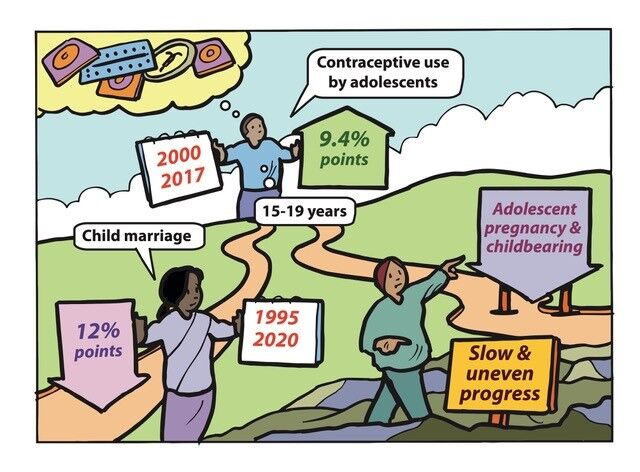
Globally the levels of adolescent pregnancy and childbearing have declined, although progress has been slow and uneven
There are also enormous variations in levels between and within countries. In LAC, for example, the estimated ABR for Nicaragua in 2021 was 85.6 per 1000 adolescent girls in 2021, compared to 24.1in Chile in the same year (1 - UNDESA, 2021). Even within countries, there are enormous variations, for example in Zambia the percentage of adolescent girls aged 15–19 who have begun childbearing (women who either have had a birth or are pregnant at the time of interview) ranged from 14.9% in Lusaka to 42.5% in the Southern Province in 2018 (2 - Zambia MOH & ICF, 2018). In the Philippines, this ranged from 3.5% in the Cordillera Administrative region to 17.9% in the Davao Peninsula region in 2017. (3 - Philippines National Demographic and Health Survey, 2017).
Globally levels of child marriage have declined and adolescent contraception use have risen.
Globally levels of child marriage have declined, and levels of contraceptive use by adolescents have risen, thereby contributing to a reduction in adolescent pregnancy and childbearing. However, progress has been slow and uneven.
Child marriage places girls at increased risk of pregnancy because girls who are married early typically have limited autonomy to influence decision-making about delaying childbearing and using contraceptives. Levels of contraceptive use among adolescents are lower than in adults both within and outside marriage/union, because of barriers both to the provision and the use of contraceptives (4- Petroni et al., 2017; 5 - UNICEF, 2021).
Declining rates of child marriage and increasing levels of use of modern contraception by adolescents have contributed to a reduction in the levels of adolescent pregnancy and childbearing. Globally, the rate of child marriage has declined over the last 25 years from 31% in 1995 to 19% in 2020 (a 12-percentage point [PP] decrease) (5 - UNICEF, 2021). Further, there has been an increase in the aggregate level of modern contraceptive use in adolescents aged 15-19 years from 17.8% in 2000-2006 to 27.2% in 2013-2017 (6 - Li et al., 2019)[1]. Also, globally, the proportion of adolescent girls aged 15–19 years whose needs for family planning were satisfied by modern methods rose from 36% to 60% between 1995 and 2020 (7 - UNICEF et al., 2020).
However, the declines in child marriage and increases in contraceptive use have been uneven across regions and between countries. Progress in child marriage has been more marked in some regions, notably in South Asia, whereas in LAC, there has been little progress (5 - UNICEF, 2021). Similarly, there is wide variation across regions with regard to the need for family planning satisfied in adolescents. While South Asia, SSA and the Middle East and North Africa have all observed steady increases in adolescent girls’ demand for family planning satisfied by modern methods, fewer than 1 in 2 adolescent girls in these regions have their demand satisfied compared to around 3 in 4 girls in LAC, Europe and Central Asia, and 88% of girls in North America (7 - UNICEF et al., 2020). These differences are reflected at the country level as well. In Cambodia, Ethiopia and Kenya, the unmet need for family planning has decreased by more than 20PP between 2000 and 2017, whereas there has been an increase of more than 10PP in Benin, Chad, Mongolia and Nigeria in the same time period (6 - Li et al., 2019).
Levels of contraceptive use among adolescents are lower than in adults both within and outside marriage/union, because of barriers both to the provision and the use of contraceptives.
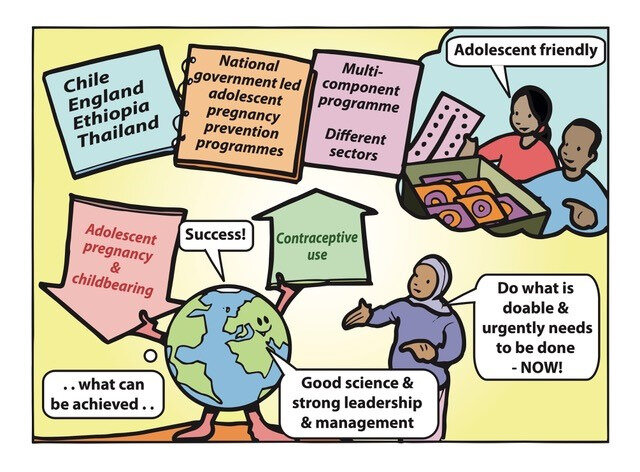
NGOs led efforts to prevent adolescent pregnancy in the past. In many countries governments are leading successful national adolescent pregnancy prevention programmes
Chile, England, Ethiopia and Thailand are part of a small but growing number of countries that have put in place successful national government-led adolescent pregnancy prevention programmes. They increased access to and uptake of contraception by adolescents through the integration of adolescent-friendly health service elements into national health systems.
For years, nongovernment organizations (NGOs) have led efforts to prevent adolescent pregnancy in countries of both the global North and the South. From their work and from research studies, there is a solid evidence base of effective approaches to prevent adolescent pregnancy and increase access to and uptake of contraceptives by adolescents. Till recently, these proven approaches were being implemented only in small-scale and time-limited projects. This is beginning to change. There is now a small but growing number of countries with successful government-led national adolescent pregnancy prevention programmes such as those in Chile, England and Ethiopia. There are valuable lessons to draw from these countries:
THEY PUT SCALE UP ON THE AGENDA: Well-connected groups of internal and external change agents worked together to create momentum for scaling-up adolescent pregnancy prevention.
THEY PLANNED SCALE UP METICULOUSLY: They developed evidence-based strategies grounded in supportive national policies. They simplified the package of interventions to only the essential elements and communicated clearly what needed to be done, where, how and by whom.
THEY PUT MONEY ON THE TABLE AND EFFECTIVELY MANAGED SCALE-UP: They committed adequate resources – from both internal and external sources in the case of Ethiopia - and managed implementation by engaging and sustaining relevant government departments at different levels, NGOs and professional associations.Further, they used findings of assessments and reviews to reshape implementation.
THEY BUILT SUPPORT AND ANTICIPATED AND ADDRESSED RESISTANCE: England and Chile anticipated resistance to providing contraception to unmarried adolescents and worked strategically to address it. Ethiopia focused on young married women whose needs were acknowledged.
THEY WORKED STRATEGICALLY TO ENSURE SUSTAINABILITY: All three countries used data creatively to communicate the progress being made. They advocated for – and succeeded in - integrating elements of the scale-up effort into wider national policies, strategies and indicator frameworks. (8 - Chandra-Mouli et al., 2019; 9 - Akwara et al., 2022; 10 - Hadley et al., 2016).
There is now a small but growing number of countries with successful government-led national adolescent pregnancy prevention programmes such as those in Chile, England and Ethiopia.
All three countries worked to integrate proven adolescent-friendly contraceptive provision elements into national health systems. For example, Chile implemented a five-pronged health systems approach:
training health workers (and providing them with clear directives on parental consent, adolescent autonomy and protection of young people from sexual abuse);
creating adolescent spaces in primary health centres;
In all three countries, efforts to expand contraceptive provision and to make it more responsive to adolescents’ needs were grounded in a broader approach delivered through multisectoral partnerships within and outside the government. For example, in England, this included the provision of comprehensive sexuality education, communication campaigns, and dedicated support for young parents[2]. (8 - Chandra-Mouli et al., 2019; 10 - Hadley et al., 2016).
The combined efforts lead to impressive results. Chile saw a 51PP reduction in the proportion of births to mothers aged under 19 years between 2000-2017 and an 8PP increase in adolescents aged 15-19 years using modern contraceptives between 2012 and 2019 in Chile. England saw a 55% reduction in the under-18 conception rate between 1998 and 2015. In Ethiopia, there was a 33.5PP increase in modern contraceptive use between 2000 and 2019; a 37.8PP increase in post-partum family planning between 2000 and 2016; a 2.9PP decrease in childbearing between 2000 and 2019 and an 8.8PP decrease in child marriage between 2000 and 2016. (8 - Chandra-Mouli al., 2019; 9 - Akwara et al., 2022; 10 - Hadley et al., 2016).
Over the years, Thailand has charted successes in many areas of public health. To address rising levels of adolescent pregnancy, Thailand put in place an Adolescent pregnancy prevention and solution initiative (2017-2026) which includes coordinated complementary actions by six government departments. Activities included the provision of sexuality education, contraceptive and safe abortion care services, social services, and community engagement, through both the public sector and business establishments. These efforts led to a huge expansion in the provision of long-acting contraceptive methods and a ten-fold increase in their uptake. This also led to reductions in adolescent pregnancy rates in 10-14-year-olds from 1.3/1000 in 2014 to 0.7/1000 in 2021, and in 15-19-year-olds from 47.8/1000 in 2014 to 32.7/1000 in 2021 (12-UNDESA, 2023).
The experiences of these countries – one each in Europe, Latin America, South Asia and sub-Saharan Africa, show what can be achieved with the application of good science combined with good evidence and strong leadership and management.They challenge and inspire other countries to do what is doable and urgently needs to be done – now.
Countries, communities and families are being left behind
Even though there has been progress globally, it has been slow and uneven, with countries, communities and families being left behind. To meet the Sustainable Development Goal’s (SDG) call of leaving no one behind, there is a pressing need to understand and address this inequity.
A recently published UNFPA report titled “Childhood in motherhood” reiterates that while progress has occurred in adolescent pregnancy and childbearing, the pace has been slow. It notes that the decline translates to about three percentage points per decade for the last six decades (13 - UNFPA, 2022). The report also points to three areas that need particular attention:
Firstly, six decades ago 14% of adolescent first births were to girls aged 14 years and younger. Recent estimates suggest that 6% of adolescent first births were to girls of this age. This important because the highest risk of maternal complications is to the youngest mothers. According to the report, the Central African Republic, Chad, and Guinea are among countries with the highest levels of births to very young mothers. Indonesia on the other hand has seen a striking decline in births among this age group over the last half-century.
Secondly, six decades ago, a girl with a first birth at the age of 14 years or younger had on an average 3 births during adolescence. Today the average has declined to 2.2. For girls with first births between 15-17 the rates have declined over 60 years from 1.9. to 1.5. According to the UNFPA report, Afghanistan, Iraq, Somalia and Nigeria are among the countries with the highest risks of repeat childbearing in adolescence. Bangladesh on the other hand has seen a marked declined in repeat childbearing during adolescence.
Thirdly, six decades ago, an adolescent mother had a one-in-three chance of having another child within two years (a rapid repeat pregnancy). Today the estimated rate is one-in-five. Rapid repeat births are associated with severe health risks to both mothers and infants. According to the UNFPA report, Jordan and Palestine see some of the highest likelihoods of rapid repeat births, whereas Brazil and Colombia have experienced some of the strongest declines in rapid repeat births to adolescents.
Beyond this, as noted above, there are huge variations in levels of adolescent pregnancy and childbearing within countries. An intersecting web of factors at the micro, meso and macro levels contribute to this (14 - Chandra-Mouli et al., 2021). Studies in SSA, LAC and South-East Asia point to adolescent first births being more common among the poorest and rural residents with births among the youngest age group (< 16 years) concentrated among these populations (15, 16, 17, 18 - Neal et al., 2016; 2018; 2019; 2020). Progress in reducing adolescent first births has been particularly poor amongst these vulnerable groups, leading to increasing inequity. For instance, in LAC, there has been little progress in reducing adolescent first births over the last few decades in Haiti (modest decline), Bolivia and the Dominican Republic (plateau in the decline), and Colombia and Peru (increase) (16 - Neal et al., 2018).
Studies in SSA, LAC and South-East Asia point to adolescent first births being more common among the poorest and rural residents with births among the youngest age group (< 16 years) concentrated among these populations.
To sum up, while there has been overall progress, there are countries,
communities and families that have been being left behind. There is a
pressing need for initiatives that seek to understand who is being left
behind, and work with them to identify why this is happening and what
can be done – with them - to address the situation.
The work of
the Women’s Centre of Jamaica (WCoJ) over four decades illustrates this
well. The WCoJ responded to the lack of opportunities for pregnant
adolescents to continue their education if they became pregnant, the
limited to no reentry opportunities for adolescent mothers, and the high
rates of second births to adolescents. The organization piloted the
provision of a package of actions to pregnant and parenting
adolescents, their male partners and their families: continued
education, counselling, school placement support, child care and
parenting skills building, and family planning counselling and service
provision, in a safe environment. With support from the Government of
Jamaica and partners both within and outside the country, the initiative
moved steadily from a pilot to a nationally scaled up programme that
has been sustained for 40 years, and replicated in other Caribbean
countries. It has also contributed to shaping national policies and
procedures on school retention and reentry for pregnant and parenting
adolescents. Finally, a body of studies have demonstrated the
effectiveness of the initiative in maintaining low levels of rapid
repeat pregnancy, and assuring school completion and continued
education (19 - Amo-Adjei et al., 2022).
To sum up, while there has been overall progress, there are countries, communities and families that have been being left behind. There is a pressing need for initiatives that seek to understand who is being left behind, and work with them to identify why this is happening and what can be done – with them - to address the situation.
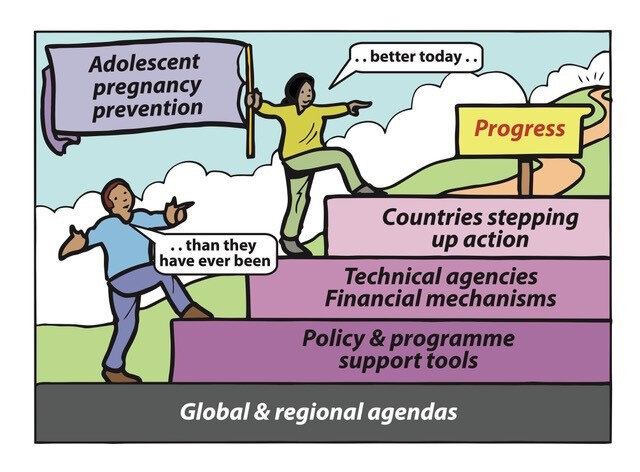
The prospects for progress on adolescent pregnancy are better today than ever before
With solid positioning on global and regional agendas, a solid and growing body of evidence feeding into norms/standards/guidelines, support from global technical support and financing mechanisms, and an increasing number of countries stepping up action, the prospects for progress are better today that they have ever been.
Adolescent pregnancy prevention is on the agenda of the Sustainable Development Goals and the International Conference on Population and Development + 25 Agenda (20 – Global SDG Indicator Platform, no date). It is also solidly positioned in the agenda of regional political bodies (21 – SRHR Score Card, no date). Over the years, a solid body of evidence on what it takes to prevent pregnancy in adolescents has been built and is being strengthened further through prospective research (22 – Pathfinder International, no date), and through retrospective documentation of noteworthy country-level initiatives (19 - Amo-Adjei et al., 2022). This evolving body of evidence and programmatic experience is informing policy and programme support tools (23 - UNFPA, 2022). Global partnerships such as FP2030 are encouraging and supporting countries to develop bold and innovative commitments (24 - FP2030, 2021).
Global financing institutions such as the Global Financing Facility are providing countries with the funds they need to translate their plans into action (25 - Global Financing Facility, 2022). They and others such as the Global Fund for AIDS Tuberculosis and Malaria are pressing for stronger synergies between HIV and early pregnancy prevention programmes (26 - The Global Fund, 2022). Global initiatives such as WHO’s Adolescent and Youth Technical Assistance Coordination Mechanism (27 - WHO, 2021/ AYSRH TA Mechanism - Review Meeting - June 2021.pdf) and The Challenge Initiative are supporting countries to translate country aspirations into context-specific programmes, delivered at scale with quality and equity, and to make full use of approaches such as Self Care and the direct-to-consumer movement (28 - Bose e al., 2021). There is much more to be done. There are both enormous opportunities to exploit and challenges to overcome but the prospects for progress are better today than they have ever been.
This is data for 43 countries with at least one survey taken in each of
the three rounds (2000-2006; 2007-2012; 2013-2017) to the same cluster
of countries in each survey round. The 43 countries are: Albania,
Armenia, Bangladesh, Belize, Benin, Burundi, Cambodia, Cameroon, Chad,
Colombia, Congo, Cuba, Côte d'Ivoire, Dominican Republic, Egypt,
Ethiopia, Ghana, Guinea, Guinea-Bissau, Guyana, Haiti, Indonesia,
Kazakhstan, Kenya, Kyrgyzstan, Lesotho, Malawi, Mali, Mongolia, Nepal,
Nigeria, Philippines, Rwanda, Senegal, Serbia, Sierra Leone, Tajikistan,
Tanzania, Thailand, Togo, Uganda, Vietnam, Zimbabwe.
In addition, in England there was open access to save abortion care and in Ethopia access to safe abortion care was liberalized.
Video message from the World Health Organization for World Contraception Day 2022
READ THE MESSAGES by the World Health Organization HERE
References
United Nations Department of Economic and Social Affairs (UNDESA). (2021) World Population Prospects, 2021 Revision: Age-specific fertility rates by region, subregion and country, 1950-2100 (births per 1,000 women) Estimates. Available at: https://population.un.org/wpp/Download/Standard/Fertility/ (Accessed 10 September 2022).
Zambia Statistics Agency, Ministry of Health (MOH) Zambia, and ICF. (2018) Zambia Demographic and Health Survey 2018. Zambia Statistics Agency, Ministry of Health, Lusaka and Rockwell.
Philippine Statistics Authority (PSA) and ICF. Philippines National Demographic and Health Survey 2017. Quezon City, Philippines, and Rockville, Maryland, USA: PSA and CF; 2018. https://psa.gov.ph/sites/default/files/PHILIPPINE%...
United Nations Children’s Fund (UNICEF). (2021) Towards Ending Child Marriage: Global trends and profiles of progress. New York: United Nations Children’s Fund, New York. https://data.unicef.org/resources/towards-ending-c...
Li Z, et al.(2019) ‘Contraceptive use in adolescent girls and adult women in low- and middle-income countries’, JAMANetwork Open, 3(2), pp. e1921437. https://pubmed.ncbi.nlm.nih.gov/32074290/
Chandra-Mouli V, et al. (2019) ‘Lessons learned from national government-led efforts to reduce adolescent pregnancy in Chile, England and Ethiopia’, Early Childhood Matters, 128, pp. 50-56. https://earlychildhoodmatters.online/2019/lessons-...
Akwara E, et al. (2022), ‘Adolescent Sexual and Reproductive Health and Rights in Ethiopia: Reviewing progress over the last 20 years and looking ahead to the next 10 years’, Reproductive Health, 19(123). https://reproductive-health-journal.biomedcentral....
Hadley A, et al. (2016) ‘Implementing the United Kingdom’s ten-year teenage pregnancy strategy for England (1999-2010): How was this done and what did it achieve?’, Reproductive Health, 13, pp.139. doi:10.1186/s12978-016-0255-4
High Impact Practices in Family Planning. (2021) Adolescent Responsive Contraceptive Services: Institutionalizing adolescent responsive elements to expand access and choice. HIP Partnership, Washington DC. https://www.fphighimpactpractices.org/briefs/adole...
UNDESA (2023). United Nations Department of
Economic and Social Affairs (UNDESA). (2023) World Population Prospects, 2022
Revision: Age-specific fertility rates by region, subregion, and country,
1950-2100 (births per 1,000 women) Estimates. Available at:
https://population.un.org/wpp/Download/Standard/Fertility/
(Accessed 30 September 2023)
Chandra-Mouli V, et al. (2021), ‘Adolescent sexual and reproductive health for all in sub-Saharan Africa: a spotlight on inequalities, Reproductive Health 18(Suppl 1), pp. 1-18. Doi: 10.1186/s12978-021-01145-4 https://reproductive-health-journal.biomedcentral....
Neal S et al. (2016) ‘Mapping adolescent first births within three east African countries using data from Demographic and Health Surveys: exploring geospatial methods to inform policy’, Reproductive Health, 13(98). doi:10.1186/s12978-016-0205-1 https://reproductive-health-journal.biomedcentral....
Neal S et al. (2018) ‘Trends in adolescent first births in five countries in Latin America and the Caribbean: disaggregated data from demographic and health surveys’, Reproductive health, 15(1), pp.146. https://reproductive-health-journal.biomedcentral....
Neal S et al. (2019) ‘Using geospatial modelling to estimate the prevalence of adolescent first births in Nepal. BMJ Global Health, 4, pp.e000763. https://gh.bmj.com/content/4/Suppl_5/e000763
Neal S, et al. (2020) ‘Trends in adolescent first births in sub-Saharan Africa: a tale of increasing inequity?’, International Journal for Equity in Health, 19(151). https://equityhealthj.biomedcentral.com/articles/1...
Amo-Adjei J., et al.(2022) ‘“Second Chances” for Adolescent Mothers: Four Decades of Insights and Lessons on Effectiveness and Scale-up of Jamaica’s PAM’,American Journal of Sexuality Education, pp. 1-34. doi:10.1080/15546128.2022.2093808
The Sexual and Reproductive Health and Rights score card for the Southern African Development Community. Available at: https://www.hera.eu/en/news/srhr_scorecard_sadc/ (Accessed: 10 September 2022).
Bose K., et al. (2021) ‘Scaling Access to Contraception for Youth in Urban Slums: The Challenge Initiative's Systems-Based Multi-Pronged Strategy for Youth-Friendly Cities’, Front Glob Womens Health, 1(2), pp.673168. doi: 10.3389/fgwh.2021.673168. https://www.frontiersin.org/articles/10.3389/fgwh....
Dr. Elsie Akwara, PhD, MPH, Independent expert. I am an experienced monitoring, data analyst and researcher in international development issues, focusing on sexual and reproductive health, gender, HIV/AIDS, maternal and child health and child protection such as child marriage. I have extensive experience in research related to measurement in adolescents and youth sexual and reproductive health (AYSRH). My work also involves qualitative content analysis, including programme and policy analysis, literature and systematic reviews, report writing and dissemination of technical content. I received my doctorate in Social Statistics and demography from the University of Southampton and Masters in Public Health at the New York Medical College. I subsequently worked at the UNFPA country office in Sierra Leone, where my primary focus was on ASRH during the Ebola period and later joined WHO as an independent consultant. Email
Dr. Venkatraman Chandra-Mouli, Scientist, Adolescent Sexual & Reproductive Health, Department of Sexual and Reproductive Health & Research, World Health Organization (which includes the UNDP/UNFPA/UNICEF/WHO/World Bank Human Reproductive Programme).
I lead the work on adolescent sexual and reproductive health (ASRH) in the Department of Reproductive Health and Research at the World Health Organization. My job is to build the epidemiological and evidence base for ASRH and to help countries translate this data and evidence into action through well-designed and well-managed policies and programmes. My experience in this field is global in scope and spans 30 years. Email