A review of abuse reported in rural Zimbabwe, before and during the COVID-19 era
Mental health in primary care
By Dr Janneke H van Dijk,
Michael Chawarika,
Talent Nyandoro,
Alvern Mutengerere,
Ehtel Manda,
Dixon Chibanda and
T. Zindava
To promote mental health care and relieve the strain on health facilities, SolidarMed Zimbabwe supported the rollout of the Friendship Bench initiative in one of the rural districts in Masvingo Province since 2019. The Friendship Bench is an intervention that deploys task shifting to address common mental disorders in Zimbabwean primary care. To understand more about the extent of the mental health burden within this rural community and explore potential gender inequalities and the impact of COVID-19 on abuse and violence, we reviewed the problem lists as presented by the clients during the lay counselling sessions.
Zimbabwe is classified as a low-income country in southern Africa with an estimated 15 million inhabitants. Most of the population (90%) is not formally employed, and poverty is endemic. The COVID-19 pandemic has further disrupted livelihoods, pushing more people into extreme poverty, with estimates of almost 49% of the population reaching extreme poverty in 2020 [World bank]. The long-lasting socio-economic challenges in the country continue to affect Zimbabwe’s health system. Government salaries are paid in the Zimbabwean currency and have severely devalued over time meaning health care workers currently receive a fraction of their previous salary. As a result, there has been an attrition of health care workers from the public sector searching for greener pastures either in the private sector or abroad, resulting in a high staff turnover. At present, many facilities are consequently understaffed, and the clinical staff remaining at the stations are often demotivated. This is further worsened by the unconducive work environment, with health facilities not able to provide some basic medical investigations as well as regular medicine stockouts at the hospital pharmacies. The result has been reduced staff commitment and poor health service delivery, and therefore quality of care.
In Zimbabwe, mental health services are skeletal, with only 13 psychiatrists for 15 million people and around 126 clinical psychologists. Services are concentrated in urban areas, yet 60% of the national population resides in rural areas. Common mental disorders (CMDs), particularly depression and anxiety, are highly prevalent across Zimbabwe, with rates of over 30% in adults attending primary health care [Chibanda et al., 2016]. CMDs are strongly associated with poverty, positive HIV status, low education, and female gender. Rural women are more predisposed to experiencing common mental health disorders because of the patriarchal norms within families and gender inequalities [Mukamana et al., 2020]. Poor access to mental health services for rural communities in Zimbabwe was confirmed by a systems analysis [Kidia et al., 2017], with identified barriers including a shortage of speciality providers, lack of funding for basic supplies and medications, and poor medication supply chains.
Primary care integration of mental health services
In rural Zimbabwe, limited to no treatment for CMDs is available, even in primary care. Unemployment is high, with most families surviving on subsistence farming and animal husbandry. Many face the challenges of intimate partner violence, substance use, and the threat or experience of political instability, in addition to the burdens of HIV and poverty. Furthermore, mental disorders are often stigmatised, particularly in hard-to-reach communities that have had little exposure to mental health education and services. The Zimbabwe National Mental Health Policy 2019-2023 and the National Mental Health Strategic Plan 2019-2023 articulate the need to integrate mental health services into primary health care as a goal and include areas that target equity in access to care. With this, increasing access to mental health services in rural areas has become a priority in Zimbabwe, though not yet (fully) achieved.
In response to this absence of mental health care services in rural Zimbabwe, SolidarMed Zimbabwe supported the rollout of the Friendship Bench (FB) initiative in Zaka district (pop. 196’323),in Masvingo Province since 2019. SolidarMed is an organisation in health, supporting the Ministry of Health and Child Care in implementing the National Health Strategy, focusing on HIV/TB, Maternal Neonatal Health, Non-Communicable Diseases, and digital health.
Masvingo province has about 10% of the country’s population. Whilst the 2nd largest psychiatric hospital in Zimbabwe lies within Masvingo province, there is no psychiatrist posted there. Only two clinical psychologists are currently operating within the province, one at the psychiatric hospital and one in private.
The friendship bench initiative - roll out in rural Zimbabwe, Zaka district.
The Friendship Bench initiative is a low-cost intervention that deploys task shifting to address common mental disorders in Zimbabwean primary care using trained and supervised lay village (community) health workers. These lay health workers are taught a structured approach to identify mild to moderate CMDs such as anxiety and depression, find workable solutions as well as detect and escalate more severe cases. After screening patients for CMDs using a validated and culturally appropriate tool – the Shona Symptom Questionnaire (SSQ-14) – the lay health workers provide a talk-therapy intervention that combines problem-solving therapy with cognitive behavioural therapy elements. After the one-on-one talk therapy, clients are invited to a peer led support group known as Circle Kubatana Tose (CKT), meaning ‘holding hands together’. This safe space contributes to the clients’ sense of belonging, reduces stigma surrounding mental health, and further allows for sharing of personal issues. In these CKT groups, clients can engage in income generating activities, relieving some economic burden. Previous trials have demonstrated that the Zimbabwean developed Friendship Bench intervention effectively addresses CMDs in a culturally appropriate way [Chibanda et al., 2016].
From early 2019 onwards, 125 VHW were trained, 5 for each of the 25 Health Facilities within Zaka district. In Zimbabwe, women represent about 70% of the health and social sector workforce and among the lay health care workers trained here, 74% were female. When people visit the Health Facility for any reason, they are invited to be screened with the SSQ tool. If a person scores above the set cut-off point, they are suggested to stay and receive the one-on-one problem-solving therapy on the “Friendship Bench”. Over the whole 2-year period since February 2019, over 14’000 people were screened using the SSQ at 23 primary care facilities and 2 district-level hospitals. Of these, over 3'500 (26%) were enrolled on the FB.
Identifying the problem
Depressed patients often initially present with aches and pains. Nurses working on the frontline were generally unsure how to make a diagnosis and focussed on the physical presentation. Physical symptoms though, especially those related to the heart and the head, can be cultural metaphors for fear or grief. For example, two main complaints: kufungisisa or ‘thinking too much’ and moyo unorwadza – 'a painful heavy heart' - implied carrying an insoluble problem and, together, seemed to encapsulate the experience of depression.
Once eligible for and interested in receiving further mental health support through the FB, clients were asked about their problems and which ones they preferred to prioritise to discuss. We categorised the problems listed, sorting those related to emotional abuse (category 1), economic abuse (category 2), physical abuse (category 3), and sexual abuse (category 4). Emotional abuse can take several forms, including accusations of cheating or other signs of jealousy and possessiveness. It can involve verbal abuse, deliberately trying to humiliate, isolate or ignore and rejection. Withholding money, stealing money, and restricting the use of finances are some examples of economic or financial abuse. It includes behaviour that denies a person economic or financial autonomy. Economic abuse often occurs in combination with other kinds of physical or emotional abuse. Physical abuse is any intentional act causing injury or trauma to another person by way of bodily contact. Sexual abuse is any unwanted sexual activity. Besides these four abuse categories, we identified three major other problem categories related to family relationships, health, and poverty.
Review of problems raised
The COVID-19 pandemic thrives on inequalities and inequities and has resulted in significant increases in gender-based violence [UN Women Africa]. Therefore, comprehending the link between any form of abuse and the COVID-19 pandemic is important in linking especially women in rural areas with the needed primary mental health services and building essential support systems.
For this purpose, we reviewed the problem lists as presented by the clients during the lay counselling sessions and reviewed the prevalence of emotional, socio-economic, physical and sexual abuse. We first reviewed data from 8 sites, including the four pilot sites where the FB was first implemented within the district and four sites included in an implementation research. Six were Rural Health Centres and 2 were Hospitals, with a total of 160-month service provision.
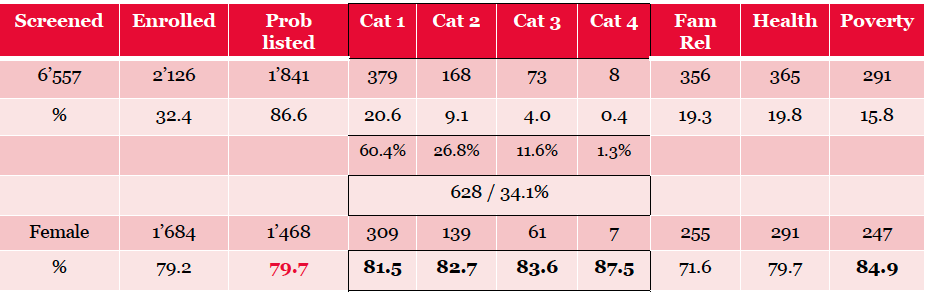
A total of 6'557 patients were screened, with 2'126 (32%) identified to have CMD. For 1'841 (86.6%) participants, the problem list was available for review. Of those, 628 (34.1%) clients raised a problem in one of the four categories of abuse. Among the abuse categories, emotional abuse was the most frequent form of abuse (60.4%), followed by economic abuse (26.8%), physical (11.6%) and sexual abuse (1.3%). Close to 80% of the clients enrolled on the FB were female, with a slightly higher proportion of females reporting abuse – ranging between 81.5% for abuse category 1 (emotional) to 87.5% for abuse category 4 (sexual).
Within the emotional abuse category, there were problems related to rejection, harassment, infidelity, and accusations.
- I am an albino, and the people are isolating me
- Being accused of being a witch
- Married in a polygamous set-up (3rd wife), facing husband and co-wives’ rejection
(problem quotes examples within the emotional abuse category)
Often people presented with several problems, which were addressed in the order the client prioritised them.For our review, in the case of abuse the highest abuse category was recorded, or in case of alternative problems, the problem that was most frequently prioritised.
- Husband does not give her money, but he wants to use her money if she does odd jobs.
- I want to kill myself because the man who impregnated me left for good, doesn’t support the child at all
- Husband does now have another wife and is no longer looking after his child
(problem quotes examples within the financial / economic abuse category)
The possible impact of COVID-19 on the problems presented
When looking at the possible impact of COVID-19 on the occurrence of abuse, we included the four pilot sites, where service provision started in Feb 2019. For these four sites, we could compare the 1-year periods of March 2019 up to February 2020 with March 2020 up to the end of February 2021. The COVID-19 pandemic reached Zimbabwe in March 2020, which was also when the first lockdowns were implemented. The four sites included one hospital and 3 Rural Health Centres.
In 2020 there was a close to 50% reduction in the number of people accessing mental health care, while the overall proportion of females enrolled on the FB stayed the same. Comparing the problem listing between 2019 and 2020, we see an overall increase in problems raised that fell within the abuse category. In 2019 about 30% of the problems presented could be categorised as abuse, whereas in 2020, this increased to 35.6%. There was an increase in the proportion of physical abuse reported within the abuse categories, whereby it seems psychological abuse escalated to a next level. Of note, people who experience physical abuse often also experience psychological and economic abuse, and there for the abuse category 3 does not exclude the existence of the lower abuse categories in the same person and does not necessarily mean a reduction in psychological abuse.
Son abuses alcohol and substances, resulting in him physically beating his parents.
My husband is harassing, beating me, and he continues to marry many wives
Being beaten by my husband claiming that the child is not his
Being beaten by the wife
(problem quotes examples within the physical abuse category 3)
Of note, the people reporting on problems related to sexual abuse were low and not allowing to comment on a change in trend during COVID-19. Reasons for not reporting sexual abuse are likely to be related to previously identified internal psychological barriers to report, including self-inflicted guilt, as well as embarrassment. In addition, as sexual abuse regularly involves intimate partners or some acquaintance, reporting of the abuse is less likely, especially in the described support set-up, whereby the Village Health Worker (VHW) potentially comes from the same community.
Husband does not want protected sex, yet his viral load is high
Raped by my grandmother’s brother
(problem quotes examples within the sexual abuse category 4)
Take home message
In conclusion, our review showed us that abuse was the most common problem listed among the people screened for CMD and enrolled for FB Mental Health services, including any or more than one of the abuse categories. During COVID-19, there was a significant reduction in access to (mental) care, while the proportion of problems listed in the abuse category increased from an overall 30 % to 36%.
As women more frequently visit the health facilities to access care for themselves or their children, they were the majority of clients seen on the Friendship Bench. As mental health services within the primary health care setting in this rural area are limited, for many of these women, the lay health care workers provided vital access to support and problem-solving therapy, providing a link to further referral as needed. Therefore the current format of service delivery allowed women to access mental health services. However, men tend to exhibit less health-seeking behaviour, leading to late detection and access to health care in general, including mental health. A different approach, possibly with a stronger community component, must be considered to improve men's use of available mental health services.
Overall, combating abuse against women is of great importance. Looking at the type of problems raised, this would need to include public education on gender relationships, increasing women's education and economic opportunities, and advocacy towards eliminating customary laws that sustain gender inequality.
Within Zimbabwe, decentralisation of mental health services to the district level and treating patients in outpatient and community-based facilities where possible, is a major goal of the National Health Policy. This decentralisation is one of the fundamental guiding principles to the sustainability of mental health, noting that it will increase access to mental health services, particularly in rural areas.
References
Chibanda et al., 2016.Dixon Chibanda1 , Helen A Weiss2 , Ruth Verhey1 ,
Victoria Simms2 , Ronald Munjoma1 , Simbarashe Rusakaniko1 , Alfred
Chingono3 , Epiphania Munetsi1 , Tarisai Bere1 , Ethel Manda1 , Melanie
Abas4 , Ricardo Araya5. Effect of a Primary Care-Based Psychological
Intervention on Symptoms of Common Mental Disorders in Zimbabwe: A
Randomized Clinical Trial. JAMA 2016 Dec 27; 316(24):2618-2626. https://jamanetwork.com/journals/jama/fullarticle/...
Kidia et al., 2017 Khameer Kidia, Debra Machando, Walter Mangezi, Reuben Hendler, Megan Crooks, Melanie Abas, Dixon Chibanda, Graham Thornicroft, Maya Semrau, Helen Jack. Mental health in Zimbabwe: A health systems analysis. The lancet Psychiatry 4(11), June 2017 – https://www.thelancet.com/action/showPdf?pii=S2215...
Mukamana et al., 2020. Iman’ishimwe Mukamana, J., Machakanja, P. & Adjei, N.K. Trends in prevalence and correlates of intimate partner violence against women in Zimbabwe, 2005–2015. BMC Int Health Hum Rights 20, 2 (2020). https://doi.org/10.1186/s12914-019-0220-
UN Women Africa. Authors/editor(s): African Union Commission (AUC), UN Women, OHCHR and UNFPA. Gender Based Violence in Africa during the COVID-19 Pandemic, 2020.https://africa.unwomen.org/en/digital-library/publ...
Dr Janneke H van Dijk, Country Director SolidarMed Zimbabwe, studied medicine in the Netherlands, where she also
obtained her DTM&H and PhD. Since 2000 she has worked as Medical
Doctor in India and Zimbabwe, and as Clinical Research Director of the
Macha Research Trust in rural Zambia. In 2015 she was appointed
Country Director of SolidarMed Zimbabwe, which has its country offices in
Masvingo – Zimbabwe, and its head-office in Lucerne, Switzerland. Email